
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Hanover, Germany, 2Department of Health Sciences and Health Policy, Faculty of Humanities and Social Sciences, University of Lucerne, Lucerne, 3Swiss Paraplegic Research (SPF), 4ICF Research Branch, a cooperation partner within the WHO Collaborating Centre for the Family of International Classifications in Germany (at DIMDI), Nottwil, Switzerland, 5Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA, USA, 6Centro de Medicina de Reabilitação da Região Centro, Tocha, 7Universidade Católica Portugesa, Medicina Dentária, Centro Regional de Viseu, Portugal and 8Graduate Program Faculty of Medicine, Universitas Gadjah Mada, Yogyakarta, Indonesia
Objective: One of the aims of the World Health Organization’s Global Disability Action Plan is to strengthen rehabilitation services. Some countries have requested support to develop (scale-up) rehabilitation services. This paper describes the measures required and how (advisory) missions can support this purpose, with the aim of developing National Disability, Health and Rehabilitation Plans.
Recommendations: It is important to clarify the involvement of governments in the mission, to define clear terms of reference, and to use a systematic pathway for situation assessment. Information must be collected regarding policies, health, disability, rehabilitation, social security systems, the need for rehabilitation, and the existing rehabilitation services and workforce. Site visits and stakeholder dialogues must be done. In order to develop a Rehabilitation Service Implementation Framework, existing rehabilitation services, workforce, and models for service implementation and development of rehabilitation professions are described. Governance, political will and a common understanding of disability and rehabilitation are crucial for implementation of the process. The recommendations of the World Report on Disability are used for reporting purposes.
Conclusion: This concept is feasible, and leads to concrete recommendations and proposals for projects and a high level of consensus stakeholders.
Key words: World Health Organization Global Disability Action Plan; National Disability Health and Rehabilitation Plan; rehabilitation advisory team.
Accepted Feb 7, 2017, Epub ahead of print April 6, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Christoph Gutenbrunner, Department of Rehabilitation Medicine, Hannover Medical School, DE-30625 Hannover, Germany. E-mail: gutenbrunner.christoph@mh-hannover.de
Approximately 1 billion people worldwide experience disability, with increasing survival rates following severe disease and trauma, increasing prevalence of chronic health conditions, and population ageing (1). The prevalence of disability is higher in low- and lower-middle- income countries. Since rehabilitation, as a health strategy, aims to enables people experiencing disability to participate fully in all areas of life (2), it is arguably the health strategy of the 21st century (3). Consequently, the World Health Organization (WHO) has identified health-related rehabilitation as an essential component of universal health coverage (4).
The United Nations Convention on the Rights of Persons with Disabilities (UNCRPD; (5)) states that access to rehabilitation is a human right. After assessing the global need for rehabilitation, the WHO has called in its Global Disability Action Plan (GDAP) 2014–2021 for action on the part of countries to “strengthen and extend rehabilitation, habilitation, assistive technology, assistance and support services, and community-based rehabilitation” (4). Countries have formally committed themselves to this goal. However, it is not always clear how countries can meet this commitment, and what measures they need to take. Provision of rehabilitation services for all people in need is a huge challenge, particularly in low- and lower-middle-income countries. Information about the prevalence of disability in these countries is poor, and their health systems are generally less developed and health resources limited. There is also a lack of standardization of rehabilitation services, which leads to problems in goal-setting and implementation planning.
The International Society of Physical and Rehabilitation Medicine (ISPRM) has made a commitment, in its formal agreement as an organization in official relationship with the WHO, to support countries “in the development of policies, strategies and plans to strengthen the provision of rehabilitation and related services by establishing Rehabilitation Advisory Teams” (ISPRM-WHO Collaboration Plan 2014–2017). The Strengthening Medical Rehabilitation Subcommittee of the ISPRM-WHO-Liaison Committee has therefore developed a framework and methodology for systematically conducting advisory missions at the country level.
This paper describes the development of principles for carrying out missions of the Rehabilitation Advisory Teams (RATs) in support of National Health, Disability and Rehabilitation Plans (NHDRPs) at the country level. Furthermore, this paper describes the development and field testing of methods for situation assessment, the development of recommendations and implementation of projects.
In the WHO GDAP 2014–2021, the objective “to strengthen and extend rehabilitation, habilitation, assistive technology, assistance and support services, and community-based rehabilitation” is made concrete in terms of the following actions (4):
Furthermore, the WHO GDAP 2014–2021 aims to strengthen research, including the life situation of persons with disabilities.
The WHO-ISPRM Collaboration Plan 2014–2017, specifies the following activities in light of the WHO agenda for rehabilitation:
Based on these questions a plan for advisory missions was developed and a Rehabilitation Service Assessment Tool (RSAT) and Rehabilitation Service Implementation Framework (RSIF) proposed. All 3 of these implementation elements were tested and refined in 2 missions that were conducted on behalf of the WHO in Egypt (6) and the Ukraine (7). An additional mission was conducted in collaboration with Handicap International (HI) in the Democratic People’s Republic of Korea (DPRK; 8).
To ensure the involvement and responsibility of national governments, WHO and the RAT, the mission was clarified by means of the terms of reference (ToR) of the mission. In order to ensure acceptance of the outcomes of the mission, a request from the government (usually, the Ministry of Health (MOH)) was sought. This request goes through the WHO country office and then to WHO headquarters in Geneva, for the attention of the coordinator of Blindness and Deafness Prevention, Disability and Rehabilitation. It might have made sense also to involve the regional offices of the WHO. In future, this pathway of requests might be modified to adapt to the situation of a specific country (for example, some steps might need to be omitted, or other relevant stakeholders or bodies involved).
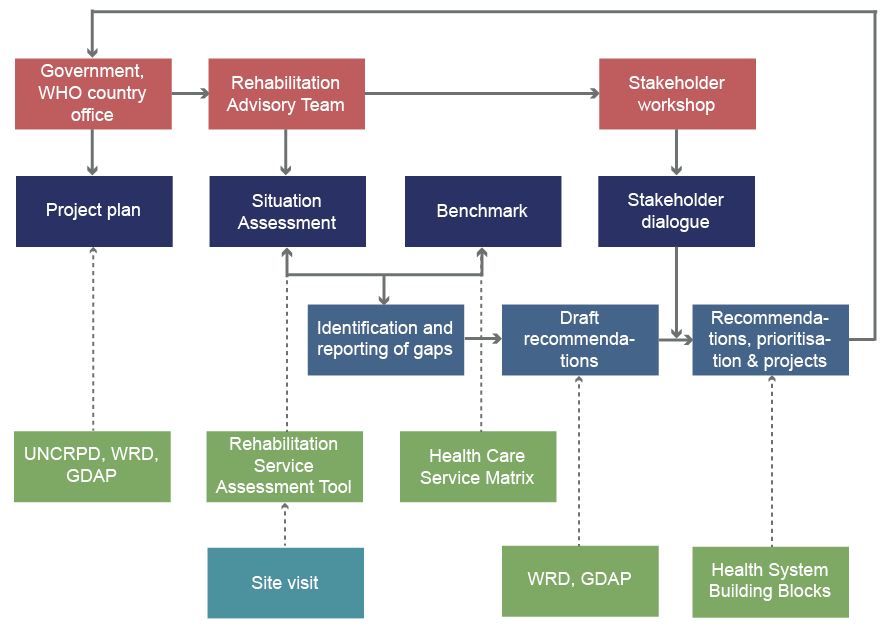
The systematic pathway for the missions (Fig. 1) describes the working steps from the project plan (prepared by the government and/or WHO country office), the situation assessments in comparison with a benchmark, the outcome in terms of identifying the gaps, and the process for developing recommendations and prioritizing them in a stakeholder dialogue. Important documents and guidelines are listed in green in Fig. 1.
Fig. 1. The process of developing National Disability, Health and Rehabilitation Plans. Red: actors; dark-blue: activities; light-blue: document development; green: guiding documents (these may change if new tools become available); blue-green: the site visit is carried out by the Rehabilitation Advisory Team (RAT) with support from the World Health Organization (WHO) country office.
The guiding principles and goals of the mission are described in the ToR. The NHDRP was developed in light of WHO GDAP objectives and based on the recommendations of the World Report on Disability (WRD) and the rights sets out in the UNCRPD. The ToR defined the method of data collection (situation analysis) and the programme and partners for the country (including government representatives, WHO experts and relevant stakeholders (in particular, organizations of people with disabilities).
The RAT includes experts with an appropriate range of knowledge, both of WHO principles and documents (such as the WRD, GDAP, and health system building blocks) and, more generally, of health systems and rehabilitation principles. The experts should also have a least practical experience in clinical and social rehabilitation and negotiation skills. It is recommended that the experts participating in the missions have an academic background, with cultural and political knowledge of the country and its health and social systems. It is also helpful if one team member is fluent in the national language; although a language barrier can also be overcome by a good interpreter.
For the recommendations it is important to collect sufficient information about relevant policies in the area of disability and rehabilitation, the need for rehabilitation at the population level, the health and social security systems, and existing rehabilitation services and workforce. Three main approaches were used to gather this information:
Searching accessible statistical sources about the population, economy, epidemiology, and health policies, and the existing rehabilitation services and workforce, including information from WHO country reports and other UN agencies (e.g. United Nations Development Programme (UNDP)/the Office of the United Nations high Commissioner for Human Rights (OHCHR)).
For site visits, it is important to ensure that existing rehabilitation services and the most important stakeholders are visited. These stakeholders are, in particular, representatives of:
The local organizer of the site visit (e.g. from the WHO country office) should ensure that the rehabilitation services visited are representative of rehabilitation services in the country. The services visited should include hospitals and rehabilitation units as well as mobile and community-based services.
The views of relevant stakeholders; not only government officials and rehabilitation professionals, but also organizations of persons with disabilities, must be involved in the information process. It is advantageous if the wider scientific community and its institutions are also involved.
Rehabilitation service implementation (as with other service implementation) is dependent on governance and political will. Implementation will be influenced by responsibilities that are sometimes split between different stakeholders and even within governments: health-related rehabilitation is often the responsibility of the MOH, while social compensation and, in many cases, delivery of assistive devices, is the responsibility of the Ministry of Social Affairs, and the training of rehabilitation professionals is the responsibility of the Ministry of Education. Thus, it is important to investigate responsibilities for rehabilitation issues across all relevant government ministries. Rehabilitation is one of the health strategies and has equal value to those of prevention, curative care and health maintenance (3). If the responsibility is split between ministries, the manner of communication and coordination between ministries is important. Finally, the RAT should have knowledge of relevant laws and regulations (both existing laws and those in preparation).
The mission depends on being aware of how disability and rehabilitation is understood at government, expert and population levels. This includes cultural norms and attitudes. It is evident in the laws and policies of many countries, as well as in how these terms are used in the local language, that they do not follow the WHO definition of disability as “the outcome of an interaction between a health condition and the person’s environment” (9). Language use often represents attitudes towards people with disabilities and understanding of disability itself.
In order to develop recommendations for service implementation, it is important to provide guidance based on scientific principles for which types of rehabilitation services are needed and how they should be organized. This also applies to the description of the field of competence of rehabilitation professionals. Such a framework or matrix is a precondition to the analysis of existing rehabilitation services and the available rehabilitation workforce. The matrix of health-related rehabilitation services developed by the authors is described in Table I.
Table I. Matrix of health-related rehabilitation services (from Gutenbrunner et al. (8); modified)
One of the most challenging issues for rehabilitation service implementation advisory missions is to systematically describe existing rehabilitation services and recommend service implementation. Due to the lack of an internationally accepted classification of rehabilitation services, Meyer et al. (10) developed a conceptual description of rehabilitation services, and Gutenbrunner et al. (11) proposed dimensions (service organization, financing and service delivery) for describing rehabilitation services. This distinction has been shown to be useful and can be used for describing or designing prototype services (12). Nonetheless, this tool cannot replace a “normative” description or classification of services. For this, some international and interdisciplinary consensus projects are necessary.
For the country mission, RAT experts chose a pragmatic approach and used a matrix in terms of primary, secondary and tertiary levels of healthcare and for all phases of care (acute, post-acute and long-term) (13). In addition, narrative descriptions of the most important types of rehabilitation services were provided (Box 1). This pragmatic approach was applicable for the development of NHDRPs. A more consensus-based service description is needed for the future (12).
Box 1. Short narrative descriptions of the most relevant types of health-related rehabilitation services (11)
A similar issue arose when describing the field of competence of rehabilitation professionals. The WHO list of health professionals has some weaknesses from the perspective of rehabilitation (14). The list does not reflect the professions identified by Neumann et al. (15) (Box 2). The definition of rehabilitation professionals from the WRD does not reflect the differentiation we believe is necessary for provision of a high-quality rehabilitation service. There is no internationally accepted description of, and curriculum for, community-based rehabilitation workers. Thus, a pragmatic approach was chosen based on a common understanding of training and professional roles of the most relevant rehabilitation professions.
Box 2. Short descriptions of rehabilitation professions and their main roles in the rehabilitation team (15)
With regard to benchmarking, no internationally accepted standards existed for the quantity and quality of rehabilitation services in health systems. From systematic research it can be recommended that health-related rehabilitation services should be integrated into the health system and financed like other (general) health services as part of the goal of universal health coverage. Thus, at present, NHDRPs cannot make quantitative recommendations for service implementation. Estimating how many services are needed to meet the needs must be part of the implementation process.
In order to achieve consensus among stakeholders of health and rehabilitation systems, the implementation tool of a stakeholder dialogue was used. This is a tool for reaching consensus for decision-making regarding policies (16, 17).
For the development of an NHDRP, the stakeholder dialogue was used to discuss the recommendations proposed by the RAT. Each recommendation was presented and briefly discussed. If there was broad agreement (>75% of participants) the recommendation was accepted. If the level of acceptance was lower a more detailed discussion was applied, the recommendation voted on again, and the result documented for the final report. In theory, recommendations with less than 25% of the vote were excluded from the final report; however, until now this has not happened, probably due to the fact that the RATs had single discussions with all stakeholders beforehand. Finally, all participants in the stakeholder workshop assigned a priority level to each recommendation. The mean priorities were set out in the final report.
For reporting purposes the decision was made about the best structure for the recommendations. The following options were considered:
For pragmatic reasons it was decided to use fewer categories (see Table II). All of the most important areas of service implementation are covered in the list. Additional categories were provided at the end after final agreement with the RAT; in 1 case the report was transformed in light of the WHO 6 health systems building blocks (18) and “synchronized” with other health system implementation activities at the country level.
Table II. Recommendations framework according of the chapter on rehabilitation of the World Report on Disability (WRD)
The plan for developing an NHDRP described here, based on the ISPRM-WHO collaboration plan, was used in Egypt (in 2015; (6)) and in the Ukraine (in 2016; (7)). Another application was conducted in collaboration with Handicap International (HI) for the DPRK (8). Summarizing these experiences, which might also be regarded as testing the underlying principles, the following conclusions can be drawn:
The resulting recommendations at the country level included the following topic areas:
Experience at the country level shows that it would be helpful if WHO headquarters, in collaboration with regional and country offices, took a strong role in the following aspects:
The application and testing of this plan for conducting missions to strengthen rehabilitation services at the country level in Egypt, Ukraine and the DPRK shows that it is feasible and can lead to concrete recommendations and proposals for projects and a high level of consensus of stakeholders. However, more projects should be carried out, and internationally agreed tools for data collection and implementation goals (i.e. model rehabilitation services and standards for rehabilitation workforce competencies) developed.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize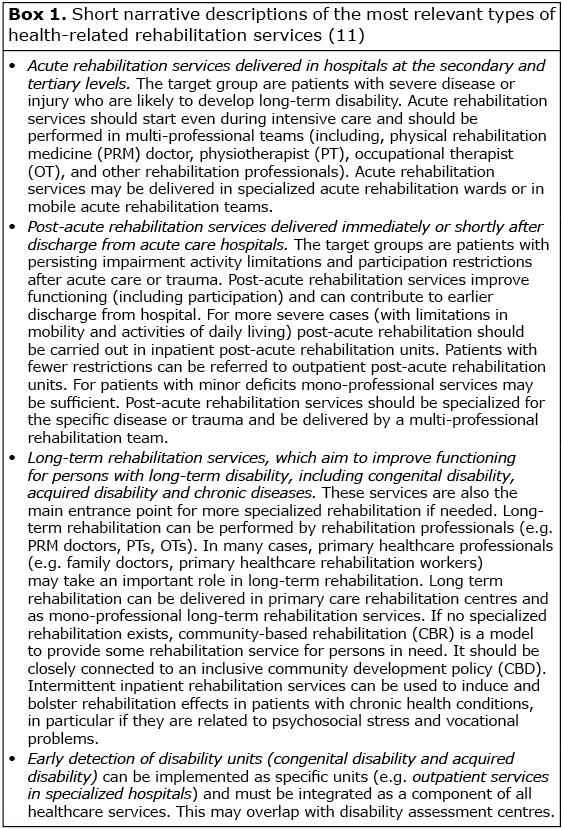 Click to show fullsize
Click to show fullsize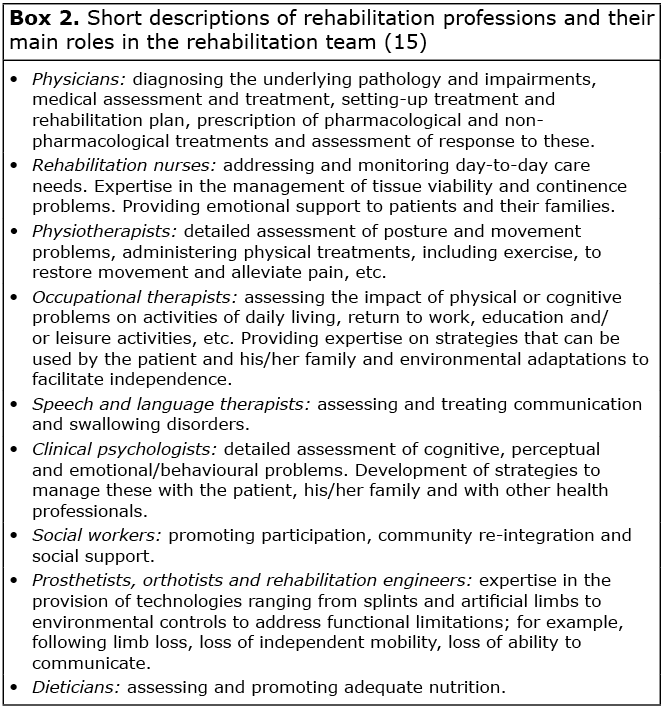 Click to show fullsize
Click to show fullsize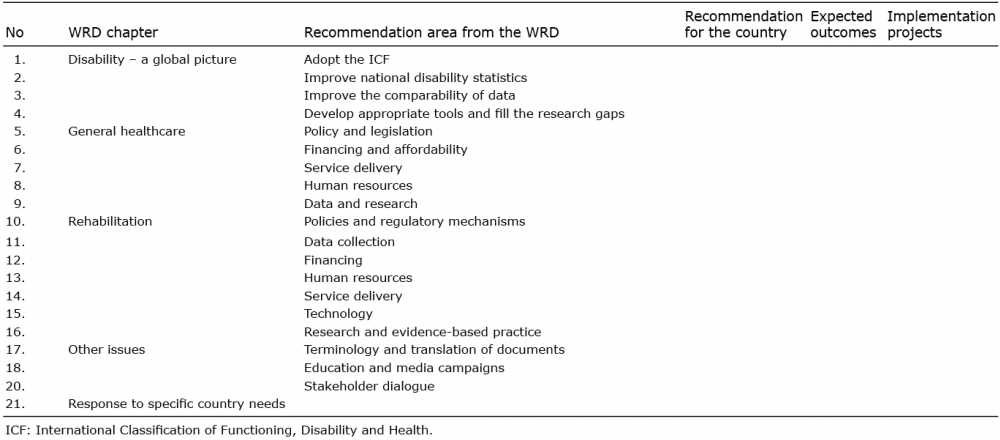 Click to show fullsize
Click to show fullsize